
FEDERATED HEALTH REGISTERS
A Literature Review
Liliana Leite
1
, Alice Miranda
1
, Carla Esteves
1
and Luis Antunes
2
1
Faculty of Medicine, University of Porto, Alameda Professor Hernâni Monteiro, 4200-319 Porto, Portugal
2
Faculty of Science, University of Porto, Rua do Campo Alegre s/n, 4169- 007 Porto, Portugal
Keywords: Federated health registers, Electronic health record, Message-based integration, Federated architecture.
Abstract: Electronic Health Records (EHR) are a collection of all individuals health data, in an electronic form,
generated during relevant interactions with the healthcare system. The federated database systems provides
intercommunication between different and autonomous data units, which enables sharing data. This paper
aims to be a state-of-art on the requirements to take into account when developing a federated system. For
that, we did a literature review on PubMed, ISI Web of Knowledge, Scopus and Google Scholar. Federated
systems must ensure interoperability using open standards; guarantee the system value through high quality
services; have modular architecture to allow developments, maintenance and evolutions, and finally, enable
the “monotonic” systems with an incremental evolution. When developing these systems we have to avoid
semantic, functional and instance conflicts to ensure the correct functionality. We concluded that federated
systems are a good option in health's domain. They allow a high volume of data storage in healthcare that
can be accessed in any place, at any time, by health professionals. Thus, we believe that federated systems
are a tool to improve the quality and efficiency of health care.
1 INTRODUCTION
With the growth of healthcare volume data at
multiples locations for a wide of users, the need for
integrate the information emerge and the concept of
Electronic Health Records (EHR) as a central
solution appears.
EHR is a collection of all individual's lifetime
health data in an electronic form produced during
relevant interactions with the healthcare system
(Tsiknakis et al., 2002). The EHR allows electronic
documentation of current and historical health like
tests, referrals and medical treatments, as well,
enable practitioners to order tests and medications
electronically. The improvement of communication
between physicians and patients is one of the
potentiality of EHRs. They can make data more
readily available, at a corporate, regional, national or
even international level. Population mobility is
increasing, and the construction of an EHR at a high
level could be an improvement for all, specially
those people.
Federation system is a process that allows
sharing information provided by different and
independent units. In health environment, the
federated approach should be capable of providing
uniform ways for accessing authentic, physician-
generated, patient record information that is
physically located in different clinical information
systems (Katehakis et al., 2001). A federated
database system is constituted by a multiple and
autonomous databases systems integrated
transparently into a single federated database. These
databases are interconnected via a computer network
and are geographically decentralize. It is a virtual
database, fully integrated, logical composite of all
constituent databases in a federated database system
(Muilu et al., 2007).
Through a literature review, we aim to study
federated electronic health records to understand this
way of sharing and archiving information.
1.1 Background
The development of federated EHR brings some
benefits (Tsiknakis et al., 2002) such as vital health
information available at any time; patient's relevant
medical history be accessed by health practitioners
what provides more efficient and effective treatment
and more quality-time with the patient; reduction of
158
Leite L., Miranda A., Esteves C. and Antunes L..
FEDERATED HEALTH REGISTERS - A Literature Review.
DOI: 10.5220/0003732401580163
In Proceedings of the International Conference on Health Informatics (HEALTHINF-2012), pages 158-163
ISBN: 978-989-8425-88-1
Copyright
c
2012 SCITEPRESS (Science and Technology Publications, Lda.)
costs and redundant procedures by accessing
information on previous medical or lab
examinations; improvement of care quality based on
an enhanced ability of health planners and
administrators to develop relevant health care
policies for the future; great empowerment of
individuals by giving them access to their own
personal health records, given them the opportunity
to exercise greater control over their own health.
Sharing medical records has the interoperability
between systems as a prerequisite and consists in a
technological chalenge (Katehakisv et al., 2001).
The implementation of such system requires
agreement between the various equipment suppliers
and will certainly increase the costs. So, the
operability of systems and services based on
standards is a key point in order to achieve the
networks’s integration of medical care (Katehakis et
al., 2001).
Modern systems are highly distributed and
heterogeneous. Interconnect data from different
sources optimize resources and enable services to
exchange information and use it in different systems
in an easier way; ensure the understanding and
preservation of the context and meaning of
information exchanged and allows coexistence of
different systems, without forcing the conversion to
a single format.
The aspects referred bellow, leads to the concept
of "interoperability" defined by Healthcare
Information Management Systems Society (HIMSS)
briefly as follows (Portuguese Health Ministry,
2009):
"Interoperability is the ability of information systems
in health work together, either within organizations
or across organizational boundaries in support of an
effective health care to individuals and the
community."
Interoperability can be materialized at various levels
like technical and semantic.
Technical interoperability ensures the integration
of different systems at the technical level,
infrastructure, media, transportation, storage and
data representation.
Semantic interoperability enables the encoding,
transmission and use of information relating to
health services among the various stakeholders,
ensuring the understanding of information, either by
their own systems, or by users.
Interoperability can be achieved by messages or
by a more advanced approach based on federated
autonomous systems (Katehakis et al., 2001). The
federated approach is used primarily to provide a
virtual view of the Integrated Electronic Health
Record (I-EHR) without replicating unnecessary
information while on the message approach there is
data redundancy.
2 METHODS
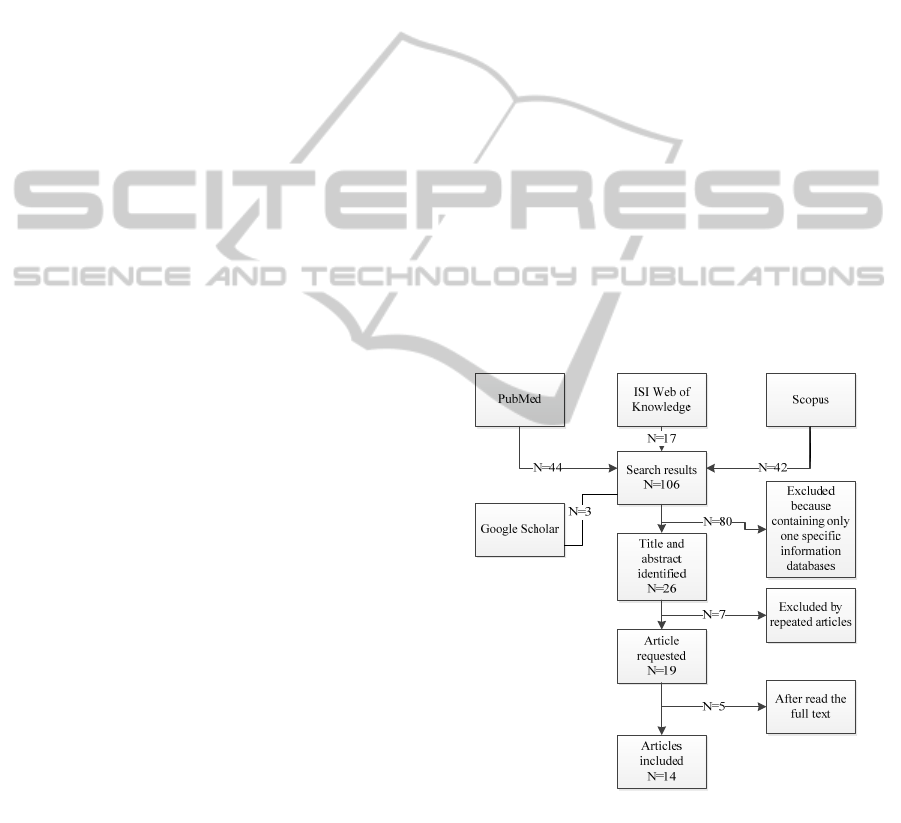
A systematic review, between 27th December 2010
and 3rd January 2011, was performed on PubMed,
ISI Web of Knowledge and Scopus. The first step
was defining our keywords: federated, health record
and health database. After combined these terms, we
construct our search query: ("federated" AND
(health record OR health database)).
Searching by article title, abstract and keywords,
it was returned 42 articles on Scopus, 17 on ISI, at
PubMed 44 articles and 3 articles on Google. After
reading the title and abstract, we excluded all the
articles containing only one specific information
databases like genome, molecular. We only choose
articles whose content was related to federated
systems focused in patient’s health history. At the
end, we selected 16, 8, 12 and 3 articles respectively.
The final result was 14 articles. The search process
is represented in Figure 1.
Figure 1: Search flow diagram.
3 RESULTS
Through a literature search, we identified some
fundamental principles that must be respected
(Katehakis et al., 2001). Federated systems must
ensure interoperability using open standards; make
FEDERATED HEALTH REGISTERS - A Literature Review
159

sure of systems value through high quality services;
have modular architecture to allow developments,
maintenance and evolutions and so, enable
“monotonic” systems with an incremental evolution.
The creation of distributed clinical information,
maintaining autonomy, needs to be tested to avoid
conflicts that can occur in three levels (table 1)
(Román et al., 2006).
Table 1: Description of problems related to the different
levels of interoperability.
Levels Description of conflict
Semantic
Originate on different databases schemas that
were created independently. Interoperability is
only possible in previously common semantic
concepts.
Functional
Different components usually have different
functionalities and interfaces. A federated system
is based in a single identification and view. The
information must be exported functionality
according to the normalized interfaces.
Instance
Happens when the same person information’s
stored in different systems has to be merged. The
corresponding Personal ID handled by each
system must be found with the guarantee that it
refers the correct person and prevent a value
conflict.
3.1 Messaging versus Federation
Interoperability between systems can be made
through messages or federation.
3.1.1 Message-based
The message-based communication, in particular
based on HL7/DICOM, is considered as a
mechanism that facilitates the functional integration
of clinical information systems and administration,
institutional or regional level, resulting in the
automation of medical processes (Katehakis et al.,
2001).
This form of messaging is mainly used to share
only portions of the I-EHR and uses various
locations to store information, what results in
redundancy of information generated (which, in
many cases, can lead to inconsistencies) because it
focuses on episodes of care and referrals and
facilitates rapid entry of data, to cover a fairly large
number of end-user requirements.
3.1.2 Federated Approach
The federated approach is mainly used to promote
the virtual view of IEHR, without information
replication.
Any federated approach to an I-EHR
environment should be able to supply uniform
means of authentication, providing quick and
authorized access to personal health records; be
physician-generated and dispose patient record
information that is physically located in a different
clinical IT system (Katehakis et al., 2001).
3.2 Reference Architecture for the
Health Information Infrastructure
(HII)
The development of global information societies led
many countries to give high priority to create and
permit access to the I-EHR of a citizen. Therefore,
another priority is the creation of a health
information infrastructure (HII) to support the
provision of a variety of telematics and healthcare
services electronically (Tsiknakis et al., 2002).
A medical institution regional/national HII is
fundamentally about bringing timely health
information and aiding communication that brings
benefits for health decisors, their families, their
patients, and their communities. By this way,
individuals and public health professionals are HII
stakeholders and users, and the applications that
meet their respective needs are important
components of the infrastructure (Tsiknakis et al.,
2002).
Taken as a whole, the HII draws upon principles,
best practices, partnerships and necessary laws, but
is based on the use of standards, systems,
applications, and technologies that support
personalized healthcare services through the
effective information integration of networked
information sources (Tsiknakis et al., 2002).
The system’s architecture is a formal description
of an IT system, organized in a way that supports
reasoning about the structural properties of the
system. It defines the components that make up the
overall information system, and provides a plan to
implement the overall system. Usually is represented
by means of an architecture model. The Reference
Model Open Distributed Processing (RM-ODP) is
an architecture model used actively by industry in
the domain of healthcare that sets a standard of
reference for an open distributed processing
(Tsiknakis et al., 2002).
The purpose, therefore, of an architecture
regarding the technical aspects for developing a HII
is to provide and enable interoperability; modularity;
migration; stability; maintenance and cost-
effectiveness.
HEALTHINF 2012 - International Conference on Health Informatics
160

3.2.1 Reference Model for Open Distributed
Processing (RM-ODP)
RM-ODP is a reference model in computer science,
which provides a coordinated framework for the
standardization of open distributed processing
(ODP). It supports distribution, interworking,
platform and technology independence and
portability, together with an enterprise architecture
framework for the specification of ODP systems.
The RM-ODP view model provides five generic and
complementary viewpoints on the system and its
environment (Tsiknakis et al., 2002).
3.2.2 Components of I-EHR
Components of I-EHR can be distinguished in
generic and specific (table 2 and 3) (Katehakis et al.,
2001); (Tsiknakis et al., 2002).
Table 2: Generic components.
Generic
components
Description
Patient
Identification (PID)
Unique association of distributed
patient record and correlating their
IDs across different clinical
information systems.
Auditing (AUD)
Record all performed interactions
between middleware services and
final-user applications.
Authentication
(AUT)
Control access.
Encryption (ENC)
Secure communications of personal
information on Virtual Private
Network (VPN) as well on the
Internet;
Resource Location
Identify availability of related
resources
Terminology (TER)
Interpret and translate terms between
different coding schemes,
terminologies and internal semantics.
User profiles (UPR)
Maintain personalized settings and
preferences
Table 3: Specific components.
Specific components Description
Indexing Service
(IS)
Primary Health
Information Access
Services
Direct access of primary healthcare
clinical systems where the complete
and original clinical information is
kept.
Update Broker
Propagation to the IS of all
modifications pertaining to clinical
information
Components like AUT, TER and REL in
conjunction with others services can be used in
implementation of structures for telemedicine, home
care, clinical messaging, etc. (Katehakis et al.,
2001).
3.3 Standardization and Projects
A large variability of institutions like IEEE (Institute
for Electrical and Electronics Engineers), WHO
(World Health Organization), ANSI (American
National Standards Institute) and ASTM
(Association for Standards and Technology
Management) are working on the production of
standards in health domain. The results were the
creation of standards like HL7 (Health Level Seven),
CEN TC251 (European Standards for Health
Informatics), ISO TC215 (International SDO for
Health Informatics), GEHR (OpenEHR) and
DICOM (Diagnostic Imaging Communications).
“The diversity of standards difficult
interoperability. Data integration from
heterogeneous sources is difficult because
information systems differ in their functionality,
terminology, semantic, interface and internal data
representation” (California Healthcare Foundation.
Clinical Data Standards Explained. November
2004).
Some European projects of federated systems are
using some standards referred before like Synapses,
a pan-European project funded under the EU Health
Telematics Programme (Grimson et al., 1998);
(Tsiknakis et al., 2002); (Bisbal et al., 2003), that is
using GEHR, CENT/TC251 (Toussaint et al., 1997).
HYGEIAnet (Katehakis et al., 2001); (Katehakis et
al., 2001) in Crete, use OMG COAS (Object
Management Group -Clinical Observation Access
Service) (Tsiknakis et al., 2002). EHR in Portugal is
using OpenEHR, HL7, DICOM, CEN/TC251 –
EN13606. Medis (Sucurovic) is a project in Serbia
and Montenegro, that develops a prototype secure
national healthcare information system; and IHE
XDS (Dogac et al., 2007) is an idea to store the
healthcare document in an ebXML
registry/repository architecture to facilitate sharing.
3.3.1 Portuguese Project
The Portuguese Electronic Health Record
(Portuguese Health Ministry, 2009) by 2015 will
incorporate issues of consolidation in Europe and it
is an example of a federated register. It’s estimated
that by 2012 it will be already in operation on a set
of public and private entities. The solution provided
by that date, will then be gradually expanded,
functional and technologically, to all healthcare
providers.
FEDERATED HEALTH REGISTERS - A Literature Review
161

This model fits into a class that may be called
"federated model" because considers a distributed
form of delivery or data repositories, both physical
and logical resources that will give body to the
whole system and considers a form of management
that provides distinct areas of authority for different
sets of information and resources, cooperating,
according to commonly accepted rules, which
compliance is subject to verification and monitoring
of a central authority.
User's Health relevant data to the I-EHR are
stored in local repositories in the entities where they
are produced, at various healthcare consultations and
occurrences;
The transaction of the identified data is made by
Push form, e.g. the different entities systems push
data to the central EHR.
Model of distributed architecture based on three
levels of aggregation and information delivery:
Level 1 (Common Core): where the information
resides (central data repository) that will be available
centrally to all users, Citizens and Healthcare
Providers, including:
- A Minimum Set of Data (Summary);
- An "index" of the clinic history of the Citizen,
which will contain links to level 2 sites, where the
information related to various episodes of care will
be stored.
Level 2 (Sharing Level): where transitional
information will be provided, standardized,
produced by a particular entity as a result of
caregiving (data conceptually divided by domains of
responsibility associated with the various entities
that at this level would provide in a standardized
manner, the relevant information).
Level 3 (Specific Level): internal level and
reserved for a particular institution, where detailed
information produced within that institution will be,
residing in their own specific systems (data stored in
the repositories of their "clinical process" place
under the jurisdiction of each entity).
Ofélia, in Portugal, is a project to manage
federated identities and authorized mechanisms.
3.4 Security of I-EHR
Healthcare is a security sensitive domain with
confidential information.
Non authorized access to medical information
violates medical confidentiality or cause alterations
of medical data that may put patient’s health at risk.
Certification of the medical identity must be
considered essential for the final granting
authentication of medical doctors and is crucial for
any federated system.
This question may be solved using some
mechanisms of protection such as digital signatures
to protect validity, authenticity and integrity of
medical information as well as non-repudiation; use
of cryptography assures confidentiality and recipient
identification. To prevent access violations a reliable
auditing mechanism has to be employed (Tsiknakis
et al., 2002).
Minimal requests to respect in a secure domain
are described (Portuguese Health Ministry, 2009):
1) Confidentiality: Must allow definition of
sensibility levels and the classification of
information in sensibility levels; ensure the
confidentiality of the information in every step of his
life cycle; need a strong encryptions mechanisms
and resent in every versions of the information.
2) Integrity: Support the existence of versions to
save and modified information.
3) Availability: Should be able the application of
physical and logical mechanisms that ensure high
level of availability when occur need of access and
utilization.
4) Identity: Require mechanisms that ensure unique
and persistently the verification of user’s identity;
verification must be ensure in a integrated way with
national identity registration; Support electronic
signature associated to each user; allows control
about user’s identity and ensure permanently
compliance of the access control laws defined;
register and alert any deviation or try of rules
violation and access mechanism in emergency
situation.
5) Access Control: Must allow a definition of
utilization profile associated to users profession and
definition of access control by each user or profile.
6) Auditability: Register, monitoring and auditing
access activity must exist in a integrate way and all
operations must be auditable and registered on
system.
4 DISCUSSION
To develop infrastructures as the Federated Health
Register is necessary overcome some challenges
(Tsiknakis et al., 2002). The first one is a
definition/adoption of federated schemas that are
capable of supporting and providing effective
solutions to immediate needs without imposing
significant constraints in dealing with the issue of
incorporating new systems in the federation. So, the
establishment of the required consent from all
HEALTHINF 2012 - International Conference on Health Informatics
162

organizational units enable exporting and mapping
of their local schema. This process involves concept
mapping, the implementation of the corresponding
data extraction gateways, and the registration of the
new feeder systems into the federation's resource
directory. This enables clinical information systems
to push information to the middle layer of the health
information infrastructure.
The use of standardized interfaces for accessing
clinical information, either directly by the end user
or through the set of components residing at the
middle level of architecture's, managing the required
minimum data sets, allows the appropriate Human
Computer Interaction environment to support easy
and efficient access to the EHR data, as well as
indexing.
The implementation of the required mechanisms
enable information consistency and guarantee the
required Quality of Service and ensure an adequate
security system, with the consent management being
part of the overall security policy.
5 CONCLUSIONS
The future challenge for researchers and system
developers (Tsiknakis et al., 2002) is to provide a
new organizational framework that possibilities
integrate a diversity of heterogeneous resources;
increase the availability of previously inaccessible
information and address the demanding information
processing requirements of modern medical
applications.
REFERENCES
Bisbal, J., J. Grimson, et al., (2003). "From passive to
active electronic healthcare records." Methods of
Information in Medicine 42(5): 535-543.
Dogac, A., G. B. Laleci, et al., (2007). "Enhancing IHE
XDS for Federated Clinical Affinity Domain Support."
Information Technology in Biomedicine, IEEE
Transactions on 11(2): 213-221.
Grimson, W., D. Berry, et al. (1998). "Federated
healthcare record server--the Synapses paradigm."
International Journal of Medical Informatics 52(1-3):
3-27.
Katehakis, D. G., S. Kostomanolakis, et al., (2001). An
open, component-based information infrastructure to
support integrated regional healthcare networks.
Medinfo 2001: Proceedings of the 10th World
Congress on Medical Informatics, Pts 1 and 2. V. L.
Patel, R. Rogers and R. Haux. 84: 18-22.
Katehakis, D. G., S. Sfakianakis, et al., (2001).
Fundamental components for the realization of a
federated Integrated Electronic Health Record
environment. Engineering in Medicine and Biology
Society, 2001. Proceedings of the 23rd Annual
International Conference of the IEEE.
Portuguese Health Ministry, Health Systems Management
Center, (2009). EHR - State of art
Portuguese Health Ministry, Health Systems Management
Center (2009). Guidelines for Functional and
Technical System of EHR.
Muilu, J., L. Peltonen, et al., (2007). "The federated
database--a basis for biobank-based post-genome
studies, integrating phenome and genome data from
600,000 twin pairs in Europe." Eur J Hum Genet
15(7): 718-723.
Román, I., L. M. Roa, et al., (2006). "Demographic
management in a federated healthcare environment."
International Journal of Medical Informatics 75(9):
671-682.
Sucurovic, S. "Implementing security in a distributed web-
based EHCR." International Journal of Medical
Informatics 76(5-6): 491-496.
Toussaint, P. J., M. Kalshoven, et al., (1997). "Supporting
shared care for diabetes patients. The synapses
solution." Proc AMIA Annu Fall Symp: 393-397.
Tsiknakis, M., D. G. Katehakis, et al., (2002). "An open,
component-based information infrastructure for
integrated health information networks." International
Journal of Medical Informatics 68(1-3): 3-26.
FEDERATED HEALTH REGISTERS - A Literature Review
163
