
DEVELOPING A WEB-BASED MIS SYSTEM FOR
OCCUPATIONAL HEALTH
Thomas M. Connolly, April MacPhail
University of the West of Scotland, High St, Paisley, Scotland, PA1 2BE, U.K.
David G. W. Scott
Sterling HealthCare, 28 Bannatyne St, Lanark, Scotland, ML11 7JR, U.K.
Keywords: Occupational Health, MIS, EHR, Interoperability, Security, Knowledge Transfer.
Abstract: Occupational Healthcare (OH) is about the promotion and maintenance of the physical, mental and social
well-being of employees. It aims to protect staff from workplace risks, but also to manage the effect of any
health issues on their work. Given the cost of absence through illness to both the organisation and the
individual, and given the government legislation that exists in this area, OH is of increasing importance to
organisations and many now outsource this service. This paper discusses how a Knowledge Transfer
Partnership (KTP) project between a university and an OH provider led to the development of a web-based
Management Information System (MIS) for Occupational Health that allows organisations to better manage
their OH provision and sickness absences. The system is currently being evaluated in a large public sector
organisation and early feedback is positive.
1 INTRODUCTION
Occupational Healthcare (OH) is about the
promotion and maintenance of the physical, mental
and social well-being of employees. It aims to
protect staff from workplace risks, but also to
manage the effect of any health issues on their work.
OH is of increasing importance to companies. For
example, in the UK each week (HSE, 2005):
one million workers take time off because of
sickness and most return to work within days;
but
around 17,000 people reach their sixth week of
statutory sick pay; and
at this point, almost one in five people will stay
off sick and eventually leave work.
Work is essential to health, well-being and self-
esteem. When ill health causes long-term sickness
absence, a downward spiral of depression, social
isolation and delayed recovery make returning to
work less likely. Reducing long-term sickness
absence helps maintain a healthy and productive
business and safeguards jobs.
While there is UK and European legislation that
makes it the responsibility of companies to ensure
the health and safety of their staff, it is also in the
companies’ best interests to look after the staff’s
health and well-being. For example, the 2008
Confederation of Business Industry (CBI) report, as
cited by Leaker (2008), found the direct cost of
absence in 2007 was £13.2 billion, around £517 for
each employee and that indirect costs added another
£263 for each employee. When these indirect costs
are added to the direct costs, the CBI estimates the
UK lost £19.9 billion to absence in 2007. In their
absence management survey report for 2009, the
Chartered Institute of Personnel and Development
(CIPD) estimated that the average cost of absence
per employee per year was £692 (£784 for public
sector employees) (CIPD, 2009) and that 7.4
working days were lost for every member of staff
per year (9.7 days for public sector organizations
and 9.4 days for non-profit organizations). Given
these statistics, it is not surprising that the market for
outsourced Occupational Health has grown in recent
years. MBD has estimated that the UK market for
OH provision grew by 34% in the period between
2003 and 2007 to a value of £394 million (MBD,
2009). In 2007, an estimated 53% of UK
occupational health services were outsourced to
private companies and MBD forecast that the UK
81
Connolly T., MacPhail A. and G. W. Scott D.
DEVELOPING A WEB-BASED MIS SYSTEM FOR OCCUPATIONAL HEALTH.
DOI: 10.5220/0002792100810088
In Proceedings of the 6th International Conference on Web Information Systems and Technology (WEBIST 2010), page
ISBN: 978-989-674-025-2
Copyright
c
2010 by SCITEPRESS – Science and Technology Publications, Lda. All rights reserved

market for OH provision will increase by 16%
between 2007 and 2012.
One approach to managing sickness absence has
been outsourcing to “Day-one” reporting systems,
which require employees who are unwell to call a
telephone number manned by OH professionals and
provide details of what is wrong with them and how
long they expect to be off. This enables the
employer to manage absence more effectively, for
instance, by arranging cover where necessary. The
service can also help employers to identify any
sickness patterns or recurring health problems with
staff. This paper discusses an alternative approach
that provides companies with an online information
system to help them manage their occupational
health requirements. In the next section, we examine
issues around the management of Electronic Health
Records (EHRs) and in Section 3 present the
requirements that have been gathered from client
companies and the key design decision for the
platform around EHRs and security. The final
section briefly provides some feedback obtained
from a first installation of the product at a large
public sector organisation in the UK.
2 PREVIOUS RESEARCH
A basic challenge of software systems in modern
medical informatics is their use of (open) standards
for communication allowing different types of
clinical applications to interact (Eichelberg et al.,
2005). Although the initial version of the platform
will be closed (ie. there will be no transfer of
information into or out of the system from or to
another external system), the company were keen
that the system would be extensible in the future.
There are a number of standards bodies in the
medical informatics area. Health Level 7 (HL7) is a
not-for-profit organisation, accredited by ANSI as a
Standards Developing Organizations (SDO) whose
specifications pertain to all aspects of clinical and
administrative data in health services. Its current
Version 3 defines (XML) messages based on a
common object-oriented Reference Information
Model (RIM) and a Clinical Document Architecture
(CDA) based on XML to specify the encoding,
structure and semantics of clinical documents for
exchange (Hooda, Dogdu, and Sunderraman, 2004).
The HL7 RIM has the following base classes
(HL7, 2009):
• Act: represents actions that have happened, are
happening, or are scheduled to happen.
• Entity: represents physical things or beings such
as persons, places, or devices.
• Role: represents the role that Entities play as
they participate in a healthcare act.
• RoleLink: represents a connection between two
Roles.
• Participation: represents the association between
a Role and an Act (for example, the context of
an Act, such as who performed it, for whom it
was performed, or where it was performed).
• ActRelationship: represents the association
between two Acts (for example, the relationship
between an order for a blood test and the result
of a blood test).
Most of these classes have subclasses that further
refine the class. For each base class in RIM, the
subclasses form a hierarchy rooted in the base class.
For example, the class LivingSubject is a subclass of
Entity, and the class Person is a subclass of
LivingSubject. Part of the RIM is shown in Figure 1.
The CDA specification states that the content of
the document consists of a mandatory textual part
(which ensures the contents are in a human readable
format) and optional structured parts (for software
processing). Different CDA levels allow for
different levels of granularity of presented clinical
information. At the simplest, level, Level One, a
document is represented through a structured header
and a body; at Level Two, sections of clinical
processes and activities have been separated by
markups; and Level Three finally provides basic
medical concepts using codification schemes such as
SNOMED (Systematized Nomenclature of
Medicine) and LOINC (Logical Observation
Identifiers Names and Codes) to represent concepts.
CDA documents are validated against the XML
schema for that level (Blobel, Engel, and Pharow,
2006).
Unlike other standards, HL7 CDA does not
specify services or protocols that are used to
exchange a document. From the perspective of HL7
messages, a CDA document is just a multimedia
object than can be exchanged as a MIME package.
openEHR (www.openehr.org) is an open
standards specification that describes the
management and storage, retrieval and exchange of
health data in Electronic Health Records (EHRs).
The primary focus of openEHR is not the exchange
of data between EHR-systems; this is the primary
focus of message standards such as HL7 and
ISO13606 (discussed shortly). openEHR has
produced a number of specifications that focus on
both the content/structure of EHRs and the
underlying technology. openEHR uses a two-level
model for EHRs: the first level, the reference model
,
provides a general framework in which any clinical
WEBIST 2010 - 6th International Conference on Web Information Systems and Technologies
82
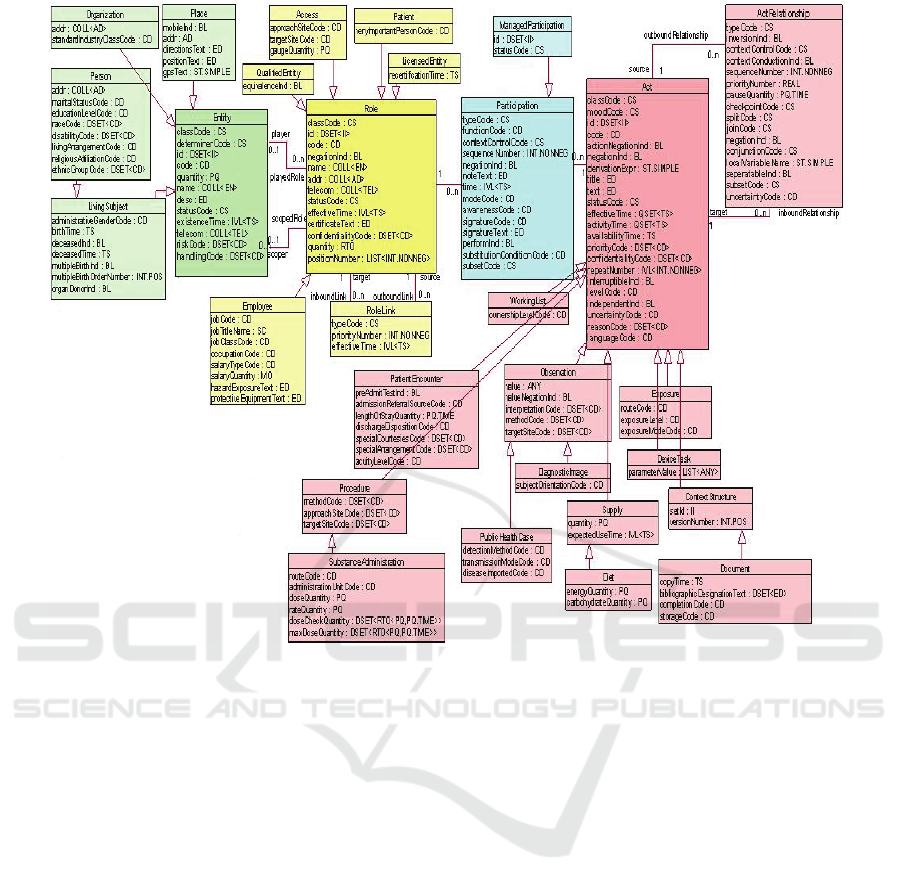
Figure 1: HL7 Reference Information Model.
information can be safely stored and exchanged; the
second level, provides rules for how specific clinical
concepts are to be used in the health record. These
rules (or archetypes) represent the clinicians’ agreed
requirements for data sharing. The reference model
specifies the overall structure of the EHR, how
contextual information is recorded, how clinical
information is organized and safely managed (Bott,
2004). Each EHR consists of a number of
compositions, which are used to capture information
around an event, such as a lab test result or a GP
appointment. The EHR can also organize these
compositions into a set of optional folders, typically
used to group events around an episode of care
Electronic Health Record Communication
(EHRCom) European Standard (EN 13606) is
another EHR specification from the technical
committee on Health Informatics of the European
Committee for Standardization (CEN/TC 251).
EHRCom is based on the older pre-standard (ENV
13606) and many concepts have been adopted from
openEHR. The standard defines an architecture for
communicating part or all of the EHRs of a single
patient, making sure that (a) the original clinical
meaning intended by the author of the record is
preserved and (b) the confidentiality of the data as
intended by the author and the patient is not
breached (Begoyan, 2008). It does not specify the
internal structure or database design/schema of the
EHR. EHRCom consists of:
The Reference Model – a generic model for
communicating part of an EHR between
heterogeneous systems;
Archetype Interchange Specification –
constraint-based approach for defining clinical
business objects that are built from the
Reference Model (adopted from openEHR);
Reference Archetypes and Term Lists – an
initial set of inter-reference model conversion
archetypes (mapping to openEHR and to the
HL7 V3);
Security Features – measures and models to
share the access control, consent and
auditability of EHR communications;
Interface Specification – message and service
interfaces to enable EHR and archetype
communication.
DEVELOPING A WEB-BASED MIS SYSTEM FOR OCCUPATIONAL HEALTH
83
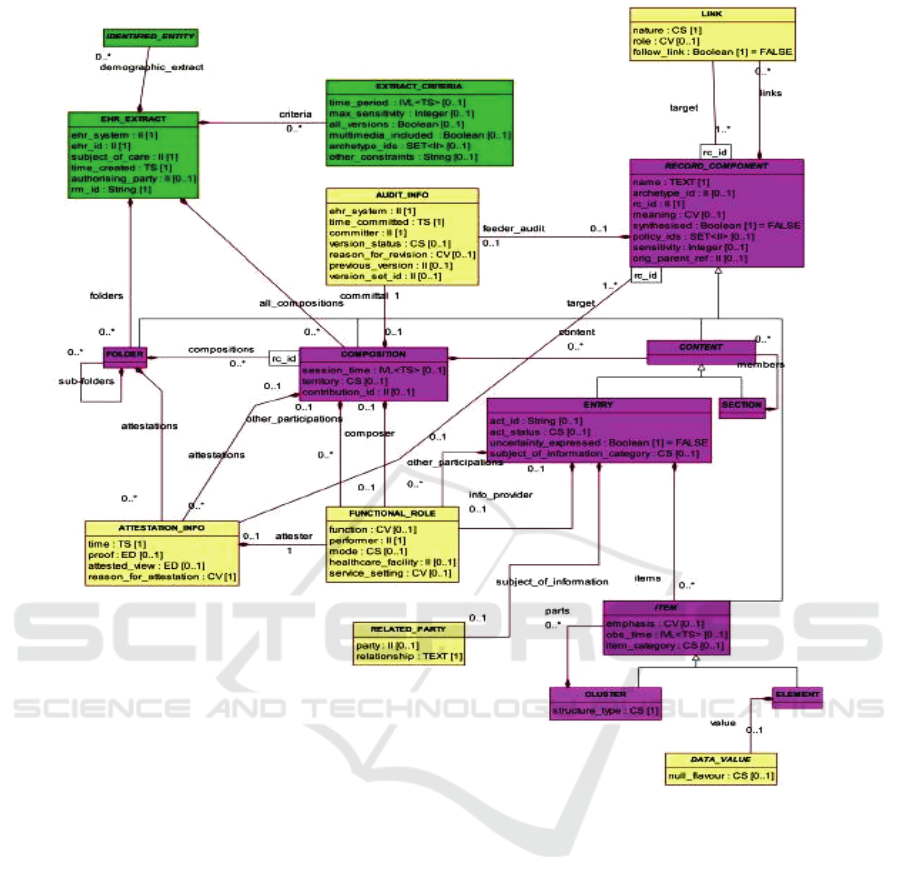
Figure 2: EN13606 Reference Model.
The EHR Reference Model defines the core
classes shown in Table 1, which closely align with
those in the openEHR Reference Model, and the
corresponding class diagram is shown in Figure 2.
As there is more than one standard, it is still
difficult to achieve interoperability. To address this
document sharing problem, an industry initiative
called Integrating the Healthcare Enterprise (IHE)
specified the Cross Enterprise Document Sharing
(XDS) Profile. The basic idea of IHE XDS is to
store healthcare documents in an ebXML registry/
repository architecture to facilitate their sharing. IHE
XDS is not concerned with document content; it
only specifies metadata to facilitate the discovery of
documents (IHE, 2009).
3 STERLING HEALTHCARE
AND STERLINGCONNECT
Sterling HealthCare is a Scottish SME that provides
an extensive range of Occupational Health,
physiotherapy and training services to match each
client’s requirements. Highly qualified OH medical
staff advise on a range of medical issues including
legislation compliance, monitoring employee health
through workplace audits and health “surveillance”,
and promoting good health at work. Sterling
HealthCare has 12.5% of the market in Scotland and
their physiotherapy division, Physicare, trade with
the majority of Local Authorities in Scotland. The
physiotherapy division also provides throughout the
UK clinics, moving and handling training and
assessment services to other public and private
WEBIST 2010 - 6th International Conference on Web Information Systems and Technologies
84
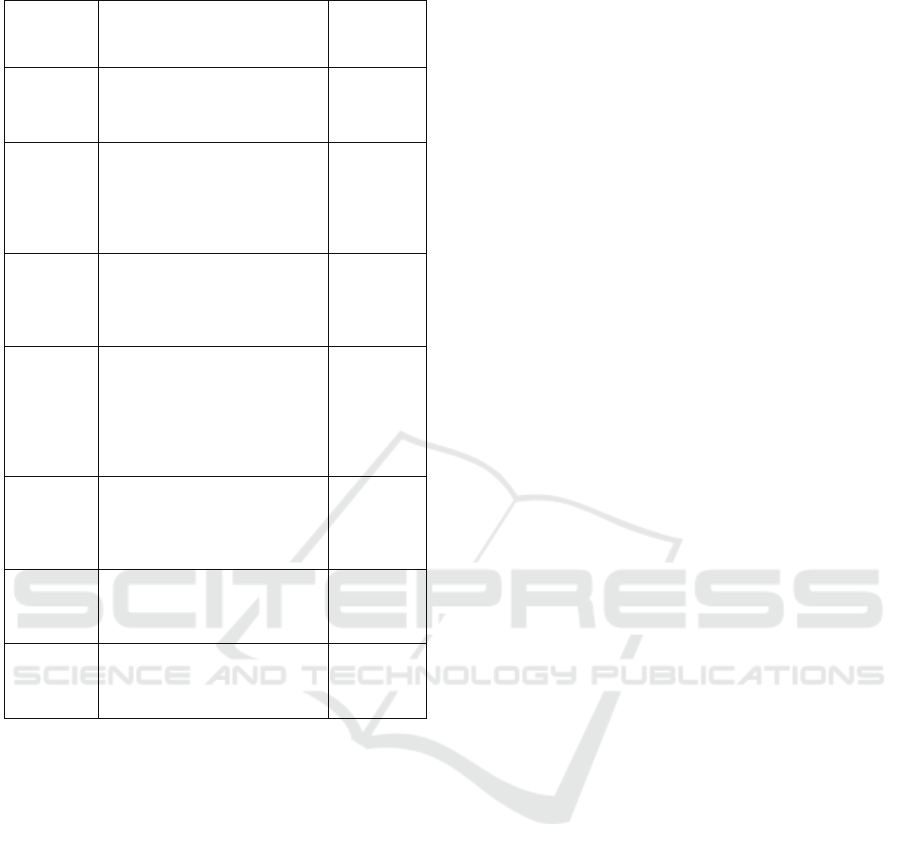
Table 1: EHR Reference Model.
EHR
Hierarchy
component
Description Examples
EHR_Extract
Top-level container of part or all of
the EHR of a single subject of care,
for communication between a
Provider and a Recipient.
Folder
High level organisation within an
EHR, with divisions related to care
p
rovided for a single condition, by
a clinical team or institution, or
over a fixed time period such as an
episode of care.
Diabetes care;
Gartnavel
Hospital, GP
Folder.
Composition
Set of information committed to
one EHR by one agent, as a result
of a single clinical encounter or
record documentation session.
Progress note;
laboratory test
results form;
referral letter;
clinic visit;
Section
EHR data within a Composition
that belongs under one clinical
heading, usually reflecting flow of
information gathering during a
clinical encounter, or structured for
the benefit of future human
readership.
Past history;
family history;
allergy
information.
Entry
Information recorded in an EHR as
a result of, for example, one
clinical action, one observation,
one clinical interpretation.
A symptom;
one test result;
a diagnosis;
b
lood pressure
measurement.
Cluster
Means of organising nested multi-
p
art data structures such as time
series, and to represent the columns
of a table.
Audiogram
results.
Element
The leaf node of the EHR
hierarchy, containing a single data
value.
Systolic blood
p
ressure; heart
rate; drug
name.
sector clients.
The company identified an opportunity to expand
its business activities but was restricted by the
limitations of the manual systems they currently had
in place. The development of a bespoke web
delivery platform (SterlingConnect) would allow
Sterling HealthCare’s clients to manage employee
absences, make OH referrals, and generally have
access to statistical information on OH data. The
platform would also allow Sterling HealthCare staff
to access and process information from any location,
thereby significantly reducing the level of
administrative staff input.
However, the company did not have the technical
knowledge to develop the system and approached a
local university to help. With funding from the UK
Technology Strategy Board through KTP
(Knowledge Transfer Partnership), the company and
the university have collaborated to develop the
system. KTP is one of Europe’s leading programmes
combining graduate recruitment with knowledge
exchange. Its benefits are proven across a range of
measures, whether company development and
profitability, knowledge exchange between
universities and business, or job creation. During the
2007/08 financial year, almost £95 million was
committed by the UK Government to new KTP
Partnerships in the form of grant support and
company contributions. At the year-end the portfolio
comprised over 1,000 individual projects, facilitating
the exchange of knowledge between the UK
knowledge base and companies across the spectrum
of size and business sector. Latest information
shows that, on average, the business benefits that
can be expected from a single KTP project are (TSB,
2008):
an increase of over £222,000 in annual profits
before tax;
creation of three new jobs;
an increase in the skills of existing staff.
A Partnership works by employing one or more
high calibre ‘Associates’ (recent graduates), to
transfer the knowledge the company is seeking into
the business. Each Associate works in the company
on a project that is core to the strategic direction of
the business. Through contact with businesses, the
knowledge base partner (academic institution) gains
relevant and improved understanding of the
challenges companies encounter which, in turn,
stimulates business-relevant teaching material and
new research themes. KTPs are an important
funding mechanism in the UK and have direct
benefits to both industry and academia, as shown in
Table 2.
3.1 Participatory Design
While Sterling HealthCare had extensive knowledge
of the OH market and their clients and staff, it was
critical that all stakeholders who would use the
system should have input into the specification of
the system requirements. Moreover, it was important
for both the company and clients that there was early
sight of the platform being developed to ensure it
met the desired requirements. As a result, it was
decided at a very early stage in the project that the
development of the platform would be underpinned
by Participatory Design principles with users and
other stakeholders playing a prominent role in all the
stages relating to design, development and
evaluation. The benefits of Participative Design are
that it can provide better project control, better
communication, more satisfied users and
participants, lessens the need for costly corrective
action post implementation and can provide more
innovative and creative solutions than might have
otherwise been possible (Kensing and Blomberg,
DEVELOPING A WEB-BASED MIS SYSTEM FOR OCCUPATIONAL HEALTH
85

Table 2: Benefits of industry/academia collaboration through KTP (adapted from Edwards, 2005).
Benefits Industry Academia
Knowledge Transfer
Acquire new knowledge and expertise Better understanding of industrial requirements and business
imperatives
Enhanced performance
Increased profitability through new
products, services and processes
Up-to-date research and teaching materials and more
relevant curriculum
Essential resource Use of high calibre personnel Increased staff
Additional finances Subsidised funding (67% for SMEs) Supplements core funding
Dissemination Publicity and promotion Learned publications
Additional opportunities
Access to wider university facilities and
potential for an on-going relationship
Student placements/projects; potential for on-going
relationship; pump-prime new research themes
1998; Cherry and Macredie, 1999).
The requirements led to the identification of the
following main subsystems: Client, Patient and
Appointments subsystem; Referral subsystem;
Occupational Health Reports subsystem; Human
Resources subsystem; security subsystem;
Electronic Health Records subsystem. The main
functionality revolves around authorised personnel
(eg. line managers and HR staff) being able to refer
their staff for an OH service.
A number of different types of referrals were to
be supported including:
Absence Management
Pre-Employment Screening
HAVS (Hand Arm Vibration Screening):
Audiometric Testing
Respiratory
Musculoskeletal
Vehicle-related (LGV; PCV; Fork Lift Driver;
Taxi Driver)
Working at Heights
Working with Lead/Asbestos.
The system maintains information on the
availability of OH professionals and OH clinics and
schedules an appointment for the referred employee
with a suitable OH professional at an appropriate
clinic (which may be within the organisation’s
premises or external to the organisation). The system
generates an email/appointment letter for the
employee. Following the consultation, the system
may schedule another appointment if the OH
professional requests it. The system generates a
letter for the employee providing a report from the
consultation, as prepared by the OH professional.
OH reports are available online for line
managers/HR to view. In addition, managers/HR are
able to view all current and historical reports/health
surveillance results on each employee, view
statistical data regarding departmental utilisation of
OH services, view OH service adherence to
performance targets, among other data. The system
will provide reminders when some action is due (eg.
an employee is due for an annual health check).
Moreover, in the UK it is a legal duty of employers
to report certain injuries/illnesses under RIDDOR
(Reporting of Injuries, Diseases and Dangerous
Occurrences Regulations) (HSE, 2008) and the
system provides advice to line managers/HR when
this occurs.
3.2 Electronic Health Records (EHR)
The storage and retrieval of EHRs was a key
component of the system and an appropriate EHR
standard had to be selected. There is some
harmonisation between the EHR standards we
examined in Section 2 (for example, the openEHR
Reference Model uses the CEN 13606 Reference
Model, which in turn is used in HL7 CDA) and
further harmonisation is likely. As a result, it was
decided to model the health records after EN 13606
and, when communication with external systems is
eventually required, to use HL7 V3 Messaging
3.3 Security
Clearly given the sensitivity of the data being stored,
security was of paramount importance in the design
of the system. Again, many of the standards
discussed in the previous section address security to
some degree. The openEHR approach to security is
based on the following two premises as proposed by
the British Medical Association (Anderson, 1996):
Informed consent: patients have a right to
expect that personal information will not be
passed on to another party unless they agree.
Relevance of access: people should only have
access to the patient’s health record if it can be
established that they are currently engaged in
provision of care for the patient, at the current
time.
In particular, privacy settings can be set on selected
parts of the EHR, not just the whole entity. There are
a number of policy principles in openEHR such as
WEBIST 2010 - 6th International Conference on Web Information Systems and Technologies
86

(Beale and Heard, 2008):
Indelibility: Health record information cannot
be deleted; logical deletion is achieved by
marking the data in such a way as to make it
appear deleted.
Audit trailing: All changes made to the EHR
including content objects as well as the EHR
status and access control objects are audit-
trailed with user identity, timestamp, reason,
optionally digital signature and relevant version
information.
Anonymity: The content of the EHR is separated
from demographic information so that theft of
the EHR provides no direct information on the
identity of the patient.
Access control lists: access should be both
relevant and time-limited (ie. during the current
period of care and possibly for some period
afterwards). An access control list can be
defined for the EHR indicating both identified
individuals and categories of users, possibly
using role types or particular staff groups. A
gate-keeper should control access to the EHR
access control settings. All changes to the list
are audit-trailed as for normal data.
Privacy: patients can mark parts (compositions)
in the EHR as having one of a number of levels
of privacy.
Other security policy principles not directly
specified by openEHR but which should be included
in an EHR deployment are:
Access Logging: Read accesses to EHR data
should be logged.
Non-repudiation: Allow digital signing of
changes to the record. Communications (EHR
Extracts) can also be digitally signed.
Certification: a mechanism should be provided
to allow a level of trust to be formally
associated with user signing keys.
The requirements around security, privacy,
confidentiality and accountability in HL7 are
extensive and include (Kratz, n.d.):
Authentication: use of Digital Signatures.
Authorization/Access Control: use of Digital
Signature, Access Control Lists.
Integrity: use of Encryption, Digital Signatures,
Check Values.
Confidentiality: use of Encryption, Key Escrow.
Accountability: use of Audit Trails, Logs, and
Receipts.
Non-repudiation: use of Encryption, Digital
Signatures.
Much of what openEHR and HL7 specify are
relevant to our system. For our (session-oriented)
application we have used SSL, SPKM, HTTP-S and
Digital Certificates. Each user has a specified
username/password and has access to a limited set of
data (eg. line managers can only access data for staff
they manage) and employees can restrict what parts
of an EHR line managers have access to. Every
record access is controlled through an access control
list and all access (including reading data) is
recorded in an audit log. No record is ever deleted
and all time-based information is maintained so that
accurate records are always available. For example,
if a medical report is prepared for an employee
called Ann Smith who subsequently marries and
changes her name to Ann Jones, at some time in the
future when the medical report is viewed again, the
original name will be shown.
3.4 Implementation
The system has been implemented in Microsoft
ASP.NET 3.5 and a centralized SQL Server 2008
database. The system is fully database driven and to
allow different clients to use different terminologies
all labels, identifiers, text and messages are taken
from the database. Similarly, all questions (eg. pre-
employment questions) are taken from the database
so that each client can modify the questions that are
asked. In effect, each web page is fully generated
dynamically at runtime. Reports are generated in
Crystal Reports. For illustration, a screen shots from
the Referral subsystem is provided in Figure 3.
Availability and reliability were key considerations
and an external hosting company was selected that
could satisfy the availability and reliability
requirements and provide an appropriate Service
Level Agreement.
Figure 3: Status of Referrals for Line Manager.
DEVELOPING A WEB-BASED MIS SYSTEM FOR OCCUPATIONAL HEALTH
87

4 CONCLUSIONS
This paper has discussed the development of a web-
based Occupational Health system and, in particular,
examining the choice of standard for storing
Electronic Health Records (EHRs). The first version
of the system has been fully tested by one of the
large Councils within Scotland with over 1,000 staff
and has been well received by all users. We
attributed the positive feedback to the use of a
Participatory Design methodology as outlined at the
start of Section 3. The main comments were around
the administration options and reports, which were
quite limited in this first version. For example, HR
wanted to be able to modify line management
arrangements (for example, an existing line manager
may leave the organisation and the staff have to be
assigned to a new line manager). In addition, the
organisation would like to be able to customise the
form data (eg. static text for labels, questions in a
pre-employment questionnaire) stored in the
database (at present, this is carried out by Sterling
HealthCare technical staff prior to installation).
Encouragingly, there have been very little comments
on the main functionality and no major bugs have
been detected. A second version of the system has
been provided with extended reporting and the
system is now in full use at the Council. It is
anticipated that the system will be rolled out to other
Councils in the UK during the first half of 2010.
The next phase is to complete the full
implementation and add enhanced administration
functions. Thereafter, an iPhone service will be
added to allow OH professionals to dictate their
findings following a consultation and for the
dictation to be stored within the employee’s EHR in
the database.
ACKNOWLEDGEMENTS
This project received financial support from the
Knowledge Transfer Partnerships programme
(KTP). KTP aims to help businesses to improve their
competitiveness and productivity through the better
use of knowledge, technology and skills that reside
within the UK Knowledge Base. KTP is funded by
the Technology Strategy Board.
REFERENCES
Anderson, R.J. 1996. A security policy model for clinical
information systems, IEEE Symposium on Security
and Privacy, 1996.
Beale, T., Heard, S. 2008. openEHR Architecture Over-
view. The openEHR Foundation, 13 November 2008.
Begoyan, A., 2007. An overview of interoperability
standards for electronic health records, Proc. 10th
World Conference on integrated design and process
technology, IDPT-2007, Society for Design and
Process Science. Antalya, Turkey, June 3-8.
Blobel, B.G., Engel, K., and Pharow, P., 2006. Semantic
interoperability—HL7 Version 3 compared to
advanced architecture standards, Methods of
Information in Medicine, 45(4), 343–353.
Bott, O.J., 2004. The Electronic Health Record –
Standardization and Implementation. In: Zywietz Ch.
(ed.): 2
nd
OpenECG Workshop Proceedings,
Integration of the ECG into the EHR &
Interoperability of ECG Device Systems. BIOSIGNA,
Berlin, 2004, 57-60.
Cherry, C., Macredie, R.D. 1999. The importance of
context within information system design: an
assessment of participative design, Requirements
Engineering, 4, 103-114.
CIPD, 2009. The CIPD Absence Management Annual
Survey Report 2009, Chartered Institute of Personnel
and Development.
Edwards, K.L., 2005. Innovation through collaboration:
Exploiting knowledge transfer in engineering product
design. In Crossing Design Boundaries, Rogers, Brod-
hurst and Hepburn (Eds). Taylor and Francis Group.
Eichelberg, M., Aden, T., Riesmeier, J., Dogac, A., Laleci,
G.B., 2005. A Survey and Analysis of Electronic
Healthcare Record Standards, ACM Computing
Surveys, 37(4), December 2005, 277–315.
HL7, 2009. HL7 Reference Information Model, Health
Level Seven, Inc., 8 June 2009, http://
ww.hl7.org/v3ballot/html/infrastructure/rim/rim.htm
Hooda, J.S., Dogdu, E., Sunderraman, R. 2004. Health
Level-7 Compliant Clinical Patient Records System.
In Proceedings of the 2004 ACM Symposium on
Applied Computing.
HSE, 2005. Working together to prevent sickness absence
becoming job loss. UK Health and Safety Executive.
HSE, 2008. A guide to the reporting of injuries, diseases
and dangerous occurrences regulations (RIDDOR)
1995. UK Health and Safety Executive, ISBN:
9780717662906.
IHE, 2009. IHE IT Infrastructure Technical Framework
Version 6.0, Cross-enterprise Document Sharing
(XDS). Integrating the Healthcare Enterprise, 10
August 2009.
Kratz, M., Humenn, P., Tucker, M., Nolte, M., Wagner,
S., Seppala, G., Shadrow, G., Wilson, W., Auton, S.
(n.d.) Health Level Seven Security Services
Framework, Health Level Seven (HL7).
Kensing, F., Blomberg, J., 1998. Participatory design:
issues and concerns. Computer Supported Cooperative
Work, 7, 167-185.
Leaker, D., 2008. Sickness absence from work in the UK,
Economic & Labour Market Review, 2(11), November
2008.
MBD, 2009. The UK Occupational Health Market Research
Report, Market and Business Development, June 2009.
TSB, 2008. Knowledge Transfer Partnerships Annual
Report 2007/08, Technology Strategy Board.
WEBIST 2010 - 6th International Conference on Web Information Systems and Technologies
88
