
Arogyashree: A Distributed File System for Large Scale
Internet-based Telemedicine
Kovendhan Ponnavaikko and D. Janakiram
Distributed and Object Systems Lab, Department of Computer Science and Engineering
Indian Institute of Technology Madras, Chennai, India
Abstract. Today, a typical telemedicine system involves a small set of hospitals
providing remote healthcare services to a small section of the society using nodal
centers, mobile health units, etc. However, the benefits of a telemedicine system
increase with scale. One of the key requirements of such a large scale system is
to allow large numbers of patient medical records, in the form of electronic files,
to be efficiently stored and accessed from widely distributed locations. In this
paper, we address the need for a distributed file system to manage patient data
in large scale telemedicine systems. We use the resources of unreliable Internet
edge nodes distributed among hospitals, labs, etc., to provide reliable file system
services to patients and doctors. Besides building an Internet-based system that
scales with the number of nodes and files, we also attempt to optimize record
access times for doctors to provide timely responses.
1 Introduction
Telemedicine is a fast evolving application that uses modern tele-communication net-
works to allow patients to be served by remotely located medical practitioners. Huge
disparities exist in the distribution of quality health care among urban and rural popula-
tions in developing countries [1]. Telemedicine has the potential to lessen this disparity.
The last decade has seen the emergence of countless telemedicine setups all around
the world [2], [3]. A typical system involves a small set of hospitals providing re-
mote healthcare services to a small section of the population using satellite technology,
nodal centers, mobile health units, etc. However, we envisage the need for much larger
Internet-based telemedicine systems at national or provincial levels.
Large scale systems enable a large pool of doctors and hospitals to collectively
provide healthcare services to entire populations. Patient records can be made accessible
to doctors from any location seamlessly. This significantly increases a patient’s chances
of receiving high quality care, since specialist doctors may sometimes not be available
nearby. Increasing mobility of doctors and patients is another reason that warrants the
need for efficient access to patient records from any location. Also, in a large setup,
patients have wider options to choose from, in terms of doctors and hospitals.
A large scale telemedicine system is capable of supporting increasing numbers of
patients and is robust against failures and attacks. Moreover, such a system can also be
Ponnavaikko K. and Janakiram D. (2009).
Arogyashree: A Distributed File System for Large Scale Internet-based Telemedicine.
In Proceedings of the 1st International Workshop on Mobilizing Health Information to Support Healthcare-related Knowledge Work, pages 105-114
DOI: 10.5220/0001819101050114
Copyright
c
SciTePress
productively integrated with third party health related systems such as national health
insurance schemes.
Management of patients’ Electronic Medical Records, or EMRs, is a key issue asso-
ciated with telemedicine [4]. A patient’s EMR may include a large variety of informa-
tion such as demographics, immunization records, history of illnesses and treatments,
allergies, pathological test results, ECGs, X-rays, etc. Though several different formats
and semantics are used by various organizations, a patient’s medical record is almost
always an ever increasing set of electronic files of various sizes.
In a large scale telemedicine system, the problem of efficiently storing and retriev-
ing EMR files of millions of patients assumes huge proportions. Storage and retrieval
of EMR files must also be done as efficiently as possible so that patients can receive
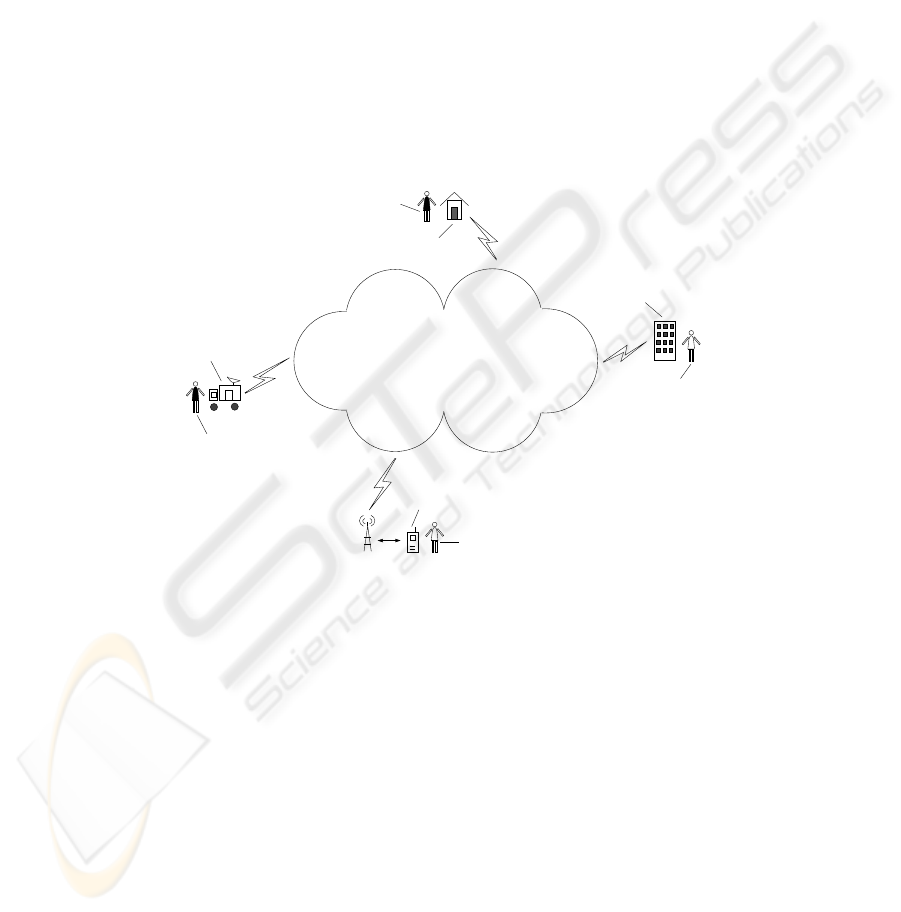
accurate and timely treatment. Arogyashree is an Internet-based Distributed File Sys-
tem (DFS) specialized to efficiently manage patient data in large scale telemedicine
projects. Figure 1 highlights some of our system features.
Doctor
Patient
Rural Health Center
Urban Hospital
Mobile Health Units
Patient
Handheld Device
Doctor on the move
Internet based File System
Widely Distributed
Large Scale
Location Sensitive
Data Placement
Fig.1. System Overview.
The requirements of our system and some related work are discussed in section 2. In
section 3, we present a few scenarios that are indicative of the purpose of Arogyashree.
Detailed description of the system follows in section 4.
2 Background and Related Work
2.1 Heterogeneity of Patient Data
These days, patient records are usually stored in multiple healthcare organizations in
different formats using different semantics. Several efforts, such as the Clinical Docu-
ment Architecture (CDA) [5], are in progress to integrate the distributed patient infor-
mation by making all the data conform to a reference architecture, such as HL7 [6]. In
106

Arogyashree, we assume that some such architecture is conformed to by all the partici-
pants.
Irrespective of the format used, patient data is almost always stored as electronic
files in the storage sites of the various healthcare organizations. For example, in the
HL7 architecture [6], CDA documents are encoded into XML [7] files with references
and links to the other medical images and multimedia files. MedGrid [8] is framework
for integrating patient information from various healthcare organizations. The frame-
work, however, uses a central registry to maintain CDA metadata, which restricts it
from scaling to billions of files.
2.2 Scalability: Usage of Internet Edge Nodes
One of the main requirements of our system is that it must scale to support a large
number of patients (order of 10
6
), and hence a large number of files (order of 10
9
).
Most of the existing solutions rely on manual data transfers. This requires users to learn
how to access each file, which is not practical.
Some distributed file systems such as NFS [9] and AFS [10] use a limited number of
servers to serve both data and metadata, severely constraining the system’s scalability.
Others such as GFS [11] and Lustre FS [12] widely distribute data serving responsibil-
ities, but use a limited number of metadata servers. Peer-to-Peer file sharing systems,
such as Kazaa [13], support dynamic environments and also scale well. However,most
such systems do not support mutable data. Doctors must not only be able to access pa-
tient files from any location, but must also be able to update the files with new results,
treatment prescriptions, etc.
We handle the issue of scale by exploiting the resources (storage, CPU, network,
etc.) of the virtually unlimited number of Internet edge nodes distributed among hos-
pitals, medical colleges, labs, healthcare organizations and even other volunteering in-
stitutions and individuals [14] to provide reliable file system services to patients and
doctors. The ubiquitous and inexpensive nature of the Internet enables such a system to
have a global reach and not be limited by even national boundaries.
Internet edge nodes are made responsible for serving both data and metadata. When
a large number of devices are used, it is critical to have efficient load balancing mech-
anisms in place to ensure that there are no potential bottlenecks in the system. Since
edge nodes can arbitrarily fail or get disconnected, the system must also incorporate
adequate fault tolerance mechanisms to render reliable file system services.
2.3 Heterogeneity and Mobility of Devices
Edge nodes can range from mobile handsets and PDAs to laptops, desktops and high-
end servers. Node availability and capabilities such as storage capacity, processing
speed, network connectivity, user interface, mobility, etc. can vary widely. The system
must take into consideration these capabilities as well as node locations while schedul-
ing data placements and accesses. Allowing mobile nodes to participate in the system
enables doctors to remain connected for longer periods of time.
107

2.4 Control over Data Placement
Data management systems such as Ceph [15] and OceanStore [16] also scale well with
large amounts of data and metadata. However, they provide little control over the kind
and location of nodes on which metadata [16] and data [15] are stored. In Arogyashree,
one of our primary concerns is to dynamically place data and metadata in appropriate
locations so that doctors can access their patients’ records without much delay. Ac-
cess time to medical records is a critical parameter that affects the performance of a
telemedicine system.
3 Indicative Scenarios
In this section, we present a few scenarios that demonstrate the usefulness of our file
system for large scale telemedicine.
Scenario One: A rural patient, P
i
, while registering with the system, will normally
prefer doctors and hospitals from nearby towns or cities to provide him/her remote med-
ical assistance. All of P
i
’s records, as and when they are generated, are then replicated
in the storage nodes at the preferred hospitals. When medical attention is required, P
i
visits a Rural Health Center (RHC) in his/her village. The practitioner at the RHC calls
the city hospital (H
c
) and makes a request for a doctor. The operator in the hospital
connects up P
i
at the RHC with the appropriate doctor at H
c
. Since all of P
i
’s EMR
is readily available at H
c
, the doctor can instantly look them up, interact with P
i
, and
prescribe the necessary treatment and medication, without encountering data transfer
delays.
Scenario Two: Suppose a patient, P
i
, is regularly treated for a cardiovascular disease
by a cardiologist, D
h
. Specialist doctors usually work at different places at different
times of the day/week. Our file system ensures that replicas of P
i
’s EMR are maintained
on (or close to) storage nodes used by D
h
. Thus, when P
i
comes to a RHC with a critical
problem, such as a cardiac arrest, D
h
, wherever he/she is, will have immediate access
to P
i
’s records with a high probability. D
h
will thus be able to quickly recommend
appropriate first aid measures and investigations.
Scenario Three: Mobile Health Units (MHU) play an important role in providing
telemedicine services to remote populations. Using satellites or other wireless commu-
nication protocols, MHUs are generally capable of connectingto the Internet. Since mo-
bile devices are also integrated into Arogyashree, MHUs can upload patient information
into the file system immediately after recording them. In several existing telemedicine
setups, medical data is sent by a MHU to a nodal hospital, where doctors have to be
present to analyze the data and recommend appropriate treatment. In Arogyashree, pa-
tient data is automatically transferred to storage nodes close to relevant doctors, rele-
vance being dictated by history, patient preference, proximity, specialization, etc. Doc-
tors can then access the records and suggest a proper course of action. Doctors on the
move can use their mobile devices to retrieve patient information and upload prescrip-
tions. Thus, rural patients can be provided specialist care instantaneously.
108

4 Arogyashree: A DFS for Large Scale Telemedicine
4.1 Clustering
The primary task of a file system for large scale telemedicine is to manage billions of
EMR files in such a way that a patient’s data is stored close to the doctors who are most
likely to treat him/her. This necessitates the usage of storage nodes close to doctors and
hospitals. Therefore, we exploit the resources of the large number of nodes, connected
to the Internet, which are distributed among hospitals, medical colleges, labs, healthcare
organizations and even other volunteering institutions and individuals to store and serve
patient files.
In order to manage the large number of nodes efficiently, system administrators
group nodes into large non-overlapping clusters (order of 10
3
nodes per cluster), based
on proximity. The cluster structure is known to the entire system (by means of well
known sites).
Every location in the geographical area (province, country, etc.) covered by the
telemedicine system is associated with one of the clusters. Hospitals, doctors and pa-
tients in a particular location, therefore, belong to the corresponding cluster, which will
be their home cluster. All of a patient’s EMR files are maintained by his/her home clus-
ter.
Clustering is done in such a way that each cluster has a sufficient number of hos-
pitals, doctors and nodes in its jurisdiction. This may require nodes in rural areas to
be clustered together with nodes in the closest urban areas (Fig. 2), since urban areas,
generally, have a much larger number of hospitals and doctors than rural areas.
Storage Node
City X
Cluster 2
Village C
Village D
Cluster 1
Cluster 3
Cluster 4
Village A
Village E
Village B
Fig.2. Clustering Example.
4.2 Two-Layered System Model
A recent approach to large scale file system organization has been to decouple file data
and metadata [11][15]. By distributing data and metadata management loads among a
109
large number of nodes, bottlenecks are prevented and system performance is enhanced.
While data refers to the actual EMR files, metadata contains useful information about
the files such as the addresses of nodes on which they are stored.
For systems handling billions of EMR files, a large number of Metadata Servers
(MDS) are required to handle the load without affecting performance. A few reliable
and capable edge nodes from each cluster are chosen to be the metadata servers for
that cluster. We call these servers Supernodes. Capabilities such as network bandwidth,
processor speed, storage space, memory capacity, etc. are used to choose supernodes.
The reliability of a storage node is measured in terms of the proportion of time the node
is reachable and available for use. As a result, static nodes are made supernodes more
often than mobile nodes, which tend to have higher disconnection rates.
Apart from being metadata servers, supernodes also monitor and manage the stor-
age nodes in their cluster. Information about patients, doctors and hospitals belonging
to their cluster are also managed by supernodes. For instance, doctors usually are asso-
ciated with a set of hospitals, use/own a set of devices, etc. Similarly, patients usually
visit a regular set of hospitals and doctors. Such information is useful for making EMR
placement decisions.
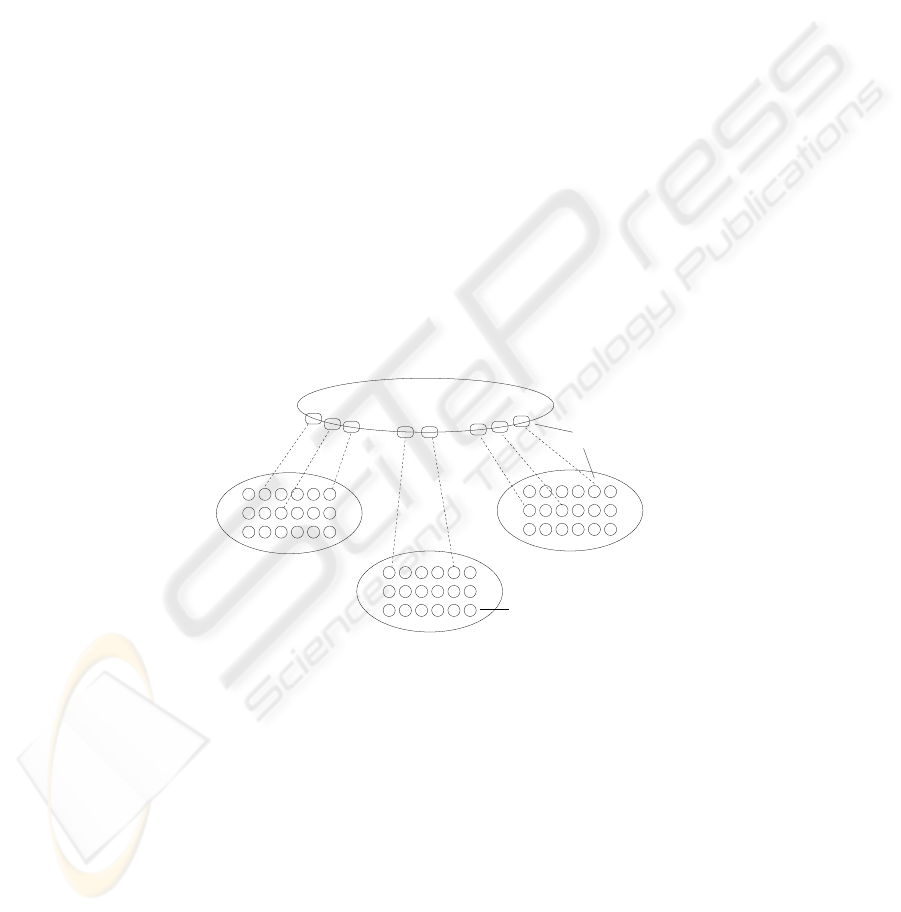
Supernodes from all the clusters form a single system-wide structured P2P overlay
network or Distributed Hash Table (DHT) [17], [18] (Fig. 3). The overlay is required to
connect up all the clusters in the system. It helps users discover the location of records
managed by other clusters, enables the efficient discovery of appropriate storage nodes
in other clusters, etc.
Node
Cluster
Supernode
Structured P2P Overlay
Fig.3. Two Layered Platform.
4.3 Load Balancing
Metadata management and resource monitoring loads within a cluster are distributed
among the cluster supernodes in accordance to their capabilities. A technique similar to
the usage of virtual servers in Chord [19] is adopted. A large virtual identifier space is
distributed among the supernodes of a cluster in accordance to their relative capabilities.
When the load on a supernode increases, the responsibility for a portion of the virtual
identifier space can be transferred from the heavily loaded supernode to a lightly loaded
110

one. We use the Paxos algorithm [20] to achieve consensus among a set of supernodes,
on the adjustment of the virtual identifier space.
The mapping between the virtual identifier space and the physical address of su-
pernodes in a cluster is made known to the entire system using the structured layer. A
file containing the association is stored in the structured layer with the cluster identifier
as the key. We will refer to this file as the supernodes map.
In order to balance load, files, nodes, patients, doctors, hospitals, etc. determine
the virtual supernode identifier with which they must associate themselves by applying
standard hash operations on their unique identifiers (name, address, location coordi-
nates, MAC address, IMEI number, file path, etc.). Entities can then use the supern-
odes map file to determine the physical address of the supernode responsible for that
virtual identifier.
Supernodes in a cluster periodically share their load information with each other.
When a supernode failure is detected or when all supernodes in a cluster are heavily
loaded, a new supernode can be added to the existing set. On the other hand, when all
the supernodes in a cluster are lightly loaded, one of the supernodes can be removed.
4.4 Fault Tolerance
In order to handle supernode failures, the metadata stored in a supernode is replicated
in a constant number (k
r
) of other supernodes. The number k
r
is selected in such a way
that the simultaneous failure of k
r
/2 supernodes within a cluster is highly improbable.
A supernode, S
n
, that updates some metadata has to multicast the changes to all its
replicas, so that the replicas are always in a state similar to that of S
n
.
Whenever the responsibility for a virtual identifier is transferred from S
i
to S
j
,
appropriate metadata transfer must happen. The metadata of all the resources that map
to that virtual identifier must be transferred from S
i
to S
j
and to S
j
’s replica set.
Storage nodes periodically send information about their vital characteristics, such
as available storage space, network connectivity, location, etc., to their corresponding
supernodes. These status messages help supernodes detect storage node failures. The
frequency with which status messages are received also helps in gauging the reliability
of a node. Cluster supernodes periodically exchange node status information among
themselves.
4.5 Security and Privacy
Patient data privacy and security are important issues in a telemedicine system. In Aro-
gyashree,differentkinds of cryptographictechniques can be used to encrypt patient data
and preserve its privacy. Standard practices such as the usage of Kerberos authentica-
tion protocols for the servers and clients to authenticate each other and establish secure
sessions, using Access Control Lists (ACLs) to restrict the usage of files, etc. can also
be adopted. The Artemis [21] project presents a mechanism for the secure transfer of
patient information between health care organizations in a Peer-to-Peer (P2P) setting.
111

4.6 File Placement
The objective of our file placement strategy is to place files at locations where they
are most often accessed. A patient’s medical records are most often accessed at the
hospitals that he/she frequents. Many a times, a patient is attended to by a regular set
of doctors from nearby locations. Thus, when a new file is added to a patient’s records,
Arogyashree attempts to replicate the file on storage nodes belonging to the hospitals
and doctors associated with the patient.
The set of hospitals and doctors a patient is associated with may change with time.
Arogyashree autonomously migrates patient records to the new locations. In order to
avoid excessive replication, replicas are maintained in the proximity of a limited set of
recently and frequently visited hospitals and doctors only.
When the ideal storage nodes do not have enough storage space, nodes nearby are
used to replicate the file. Network coordinates are used to discover proximal nodes.
We employ Vivaldi [22], a decentralized network coordinate system, to assign network
coordinates to storage nodes. We require only an approximate estimate of network dis-
tances to discover nearby storage nodes. Therefore, the accuracy provided by Vivaldi
[23] is sufficient for our purpose. Vivaldi vertices consist of Euclidean coordinates aug-
mented with a height and can be represented as (x, y, h). Network distance (or round
trip time) between nodes is calculated in a way similar to Euclidean distance measure-
ment. Mobile devices may need to maintain more than one set of coordinates, since
their latencies from other nodes may vary based on their location and the connection
used (WiFi, cellular network, WiMAX, etc.).
h
x
y
Fig.4. Location Space Partitioning.
In each cluster, supernodes take responsibility for different blocks of the coordinate
space. The distribution is done using hash functions, as discussed in section 4.3. Each
block is uniquely identified by the endpoints of its diagonal (Fig. 4). The list of cluster
nodes in a block is maintained by the corresponding supernode. Nodes proximal to a
particular node can then be found using simple geometric algorithms.
Supernodes ensure that files are replicated in a minimum number of storage nodes
with reasonable reliability measures. When failed nodes remain inaccessible for abnor-
mally long periods of time, their contents are replicated in other nodes. An outline of
the replica placement mechanism is shown in figure 5.
112
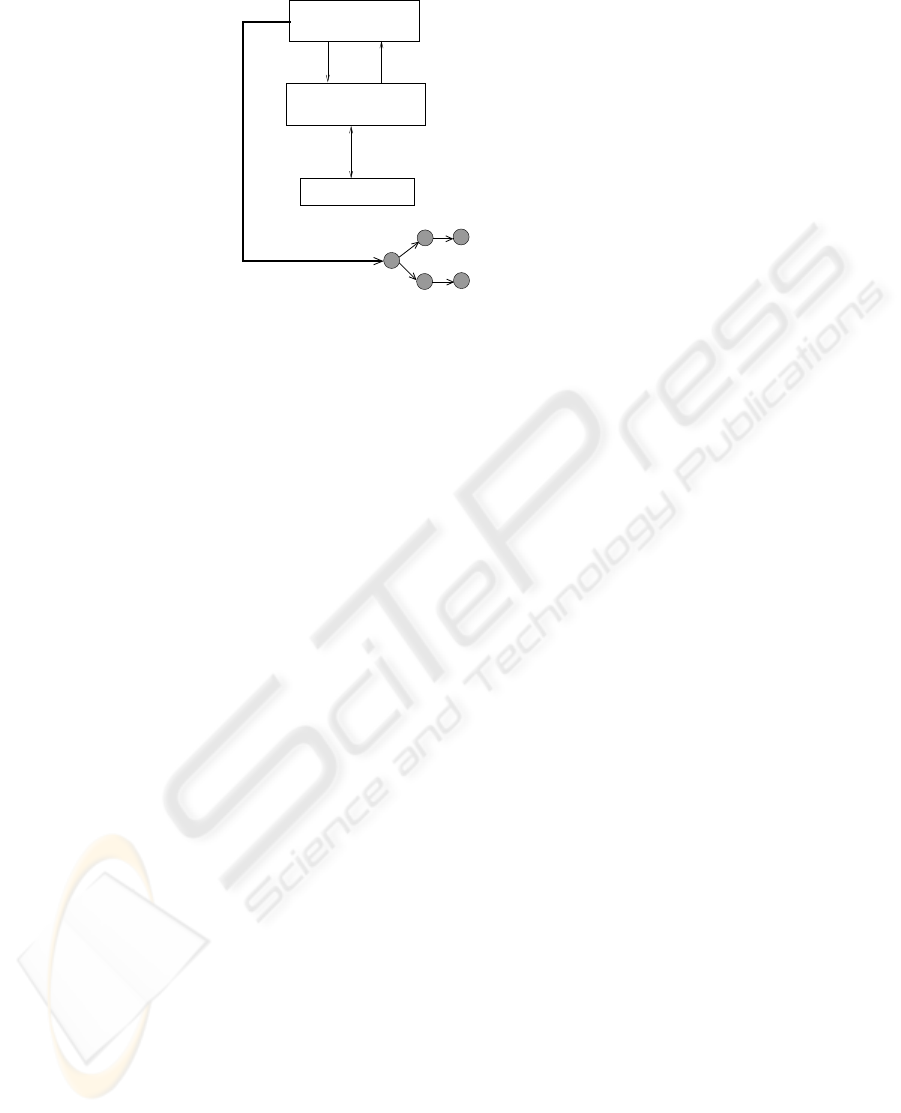
associated hospitals, doctors, nodes, etc.
Interacts with supernodes responsible for P,
1
2
3
using a
multicast tree
File transfer
4
Storage Nodes
Insert file F into
patient P’s EMR
Contact
Responds with replica locations
Supernode S
(responsible for file F)
Other Supernodes
Fig.5. Replica Placement.
5 Conclusions
In this paper, we discuss the design of a distributed file system suitable for large scale
Internet-based telemedicine projects. Arogyashree uses the resources of large numbers
of unreliable Internet edge nodes to providereliable file services to doctors and patients.
A two layered platform, comprising of clusters of proximal nodes and a system-wide
DHT, enables the distribution of metadata and data management loads among the edge
nodes. The working of our system assists in optimizing EMR access times, which is a
critical parameter that affects the performance of a telemedicine system. At our lab, we
are currently implementing a prototype model of Arogyashree as part of a sponsored
project. The prototype will be used for the evaluation of the system’s performance and
scalability.
Acknowledgements
We thank Intel Research and Indian Council of Medical Research for supporting this
work.
References
1. Bagchi, S.: Telemedicine in rural India. PLoS Medicine 3 (2006)
2. Website: Belgium-hf. (http://www.belgium-hf.be/)
3. Website: Center for connected health. (http://www.connected-health.org/)
4. Fraser, H. S., Biondich, P., Moodley, D., Choi, S., Mamlin, B. W., Szolovits, P.: Implement-
ing electronic medical record systems in developing countries. Informatics in Primary Care
13 (2005)
5. Kim, H.S., Tran, T., Cho, H.: A Clinical Document Architecture (CDA) to generate clini-
cal documents within a hospital information system for e-healthcare services. In: CIT ’06:
Proceedings of the Sixth IEEE International Conference on Computer and Information Tech-
nology, Washington, DC, USA, IEEE Computer Society (2006) 254
113

6. Dolin, R.H., Alschuler, L., Boyer, S., Beebe, C., Behlen, F.M., Biron, P.V., Shabo Shvo, A.:
HL7 clinical document architecture, release 2. J Am Med Inform Assoc 13 (2006) 30–39
7. Bray, T., Paoli, J., Sperberg-Mcqueen, C.M., Maler, E.: Extensible Markup Language (XML)
1.0 (Fourth Edition). Technical report, W3C (2006)
8. Papadakis, I., Poulymenopoulou, M.: Medgrid: A semantic-capable grid for medical data.
The Journal on Information Technology in Healthcare 4 (2006)
9. Sandberg, R., Goldberg, D., Kleiman, S., Walsh, D., Lyon, B.: Design and implementation
of the Sun Network Filesystem. In: Proc. Summer 1985 USENIX Conf. (1985) 119–130
10. Howard, J.H.: On overview of the Andrew File System. In: USENIX Winter. (1988) 23–26
11. Ghemawat, S., Gobioff, H., Leung, S.T.: The Google File System. SIGOPS OSR 37 (2003)
29–43
12. Schwan, P.: Lustre: Building a file system for 1000-node clusters. In: Proc. of Linux Sym-
posium. (2003) 380–386
13. Website: Kazaa. (http://www.kazaa.org/)
14. Sarmenta, L.F.G.: Bayanihan: Web-based volunteer computing using java. In: In Second
International Conference on World-Wide Computing and its Applications. (1998) 444–461
15. Weil, S.A., Brandt, S.A., Miller, E.L., Long, D.D.E., Maltzahn, C.: Ceph: A scalable, high-
performance distributed file system. In: OSDI. (2006) 307–320
16. Kubiatowicz, J., Bindel, D., Chen, Y., Czerwinski, S., Eaton, P., Geels, D., Gummadi, R.,
Rhea, S., Weatherspoon, H., Wells, C., Zhao, B.: Oceanstore: An architecture for global-
scale persistent storage. SIGARCH Comput. Archit. News 28 (2000) 190–201
17. Stoica, I., Morris, R., Karger, D., Kaashoek, F.M., Balakrishnan, H.: Chord: A scalable
peer-to-peer lookup service for Internet applications. In: Proc. of ACM SIGCOMM ’01.
Volume 31. (2001) 149–160
18. Rowstron, A., Druschel, P.: Pastry: Scalable, decentralized object location and routing for
large-scale peer-to-peer systems. In: Middleware ’01. (2001) 329–350
19. Rao, A., Lakshminarayanan, K., Surana, S., Karp, R.M., Stoica, I.: Load balancing in struc-
tured P2P systems. In: Proc. of IPTPS 2003. (2003) 68–79
20. Lamport, L.: The part-time parliament. Trans. Comput. Syst 16 (1998) 133–169
21. Boniface, M.J., Wilken, P.: Artemis: Towards a secure interoperability infrastructure for
healthcare information systems. In: HealthGrid 2005. (2005)
22. Dabek, F., Cox, R., Kaashoek, F., Morris, R.: Vivaldi: A decentralized network coordinate
system. In: Proc. of the ACM SIGCOMM’04 Conference. (2004) 15–26
23. Lua, E.K., Griffin, T., Pias, M., Zheng, H., Crowcroft, J.: On the accuracy of embeddings for
internet coordinate systems. In: Proc. of the 5th ACM SIGCOMM conference on Internet
Measurement, Berkeley, CA, USA, USENIX Association (2005) 11–11
114
