
MEDICAL DIAGNOSIS ASSISTANT BASED
ON CATEGORY RANKING
Fernando Ruiz-Rico, Jose Luis Vicedo and Mar´ıa-Consuelo Rubio-S´anchez
University of Alicante, Spain
Keywords:
Medical diagnosis, category ranking.
Abstract:
This paper presents a real-world application for assisting medical diagnosis which relies on the exclusive use
of machine learning techniques. We have automatically processed an extensive biomedical literature to train
a categorization algorithm in order to provide it with the capability of matching symptoms to MeSH diseases
descriptors. To interact with the classifier, we have developed a web interface so that professionals in medicine
can easily get some help in their diagnostical decisions. We also demonstrate the effectiveness of this approach
with a test set containing several hundreds of real clinical histories. A full operative version can be accessed
on-line through the following site: www.dlsi.ua.es/omda/index.php.
1 INTRODUCTION
Text categorization consists of automatically assign-
ing documents to pre-defined classes. It has been ex-
tensively applied to many fields such as search en-
gines, spam filtering, etc. and in particular, some ef-
forts have been focused on MEDLINE abstracts clas-
sification (Ibushi et al., 1999). However, as far as we
are concerned, it has never been used to assist medical
diagnosing by using the textual information provided
by biomedical literature together with patient histo-
ries.
Every year, thousands of documents are added to
the National Library of Medicine and the National In-
stitutes of Health databases
1
. Most of them have been
manually indexed by assigning each document to one
or several entries in a controlled vocabulary called
MeSH
2
(Medical Subject Headings). The MeSH tree
is a hierarchical structure of medical terms which are
used to define the main subjects that a medical arti-
cle or report is about. Due to the wide use of this
terminology, we can find translations into several lan-
guages such as Portuguese and Spanish (i.e. DeCS
3
- Health Science Descriptors). The diseases sub-tree
not only defines on its own more than 4,000 patho-
logical states, but also offers the chance to search for
documented case reports related to each of them.
1
http://www.pubmed.gov
2
http://www.nlm.nih.gov/mesh
3
http://decs.bvs.br/I/homepagei.htm
Our proposal tries to estimate a ranked list of diag-
noses from a patient history. To tackle this problem,
we haveselected an existing categorization algorithm,
and we have trained it using the textual information
provided by lots of previously reported cases. This
way, a detailed symptomatic description is sufficient
to obtain a list of possible diseases, along with an es-
timation of probabilities.
We have not used binary decisions from binary
categorization methods, since they might leave some
interesting MeSH entries out, which should probably
be taken into consideration. Instead, we have chosen
a category ranking algorithm to obtain an ordered list
of all possible diagnoses so that the user can finally
decide which of them better suits the clinical history.
In this paper, first of all, we will explain the way
we have developed our experiments, including a full
description of the sources and methods used to get
both training and test data. Secondly, we will provide
an example of a patient history and both the expected
and provided diagnoses. We will finish by showing
and commenting several evaluation results on.
2 PROCEDURES
We have extracted the training data from the PubMed
database
1
by selecting every case reports on diseases
written in English including abstract and related to
humans beings. These documents were retrieved by
using the “diseases category[MAJR]” query, where
239
Ruiz-Rico F., Luis Vicedo J. and Rubio-S
´
anchez M. (2008).
MEDICAL DIAGNOSIS ASSISTANT BASED ON CATEGORY RANKING.
In Proceedings of the First International Conference on Health Informatics, pages 239-241
Copyright
c
SciTePress
[MAJR] stands for “MeSH Major Topic”, asking the
system for retrieving only documents whose subject is
mainly a disease. The query provided us with 483,726
documents
4
that we downloaded by sending them to
a file in MEDLINE format. We automatically pro-
cessed that file to obtain the titles and abstracts with
their correspondingMeSH topics. This led us to 4,024
classes with at least one training sample each.
With respect to the test set, we have used 400 med-
ical histories from the School of Medicine of the Uni-
versity of Pittsburgh (Department of Pathology
5
). Al-
though, so far the web page contains 500 histories
4
,
not all of them are suitable for our purposes. There
are some which do not provide a concrete diagnosis
but only a discussion about the case, and some others
do not have a direct matching to the MeSH tree. We
downloaded the HTML cases and afterwards we con-
verted them to text format by using from each doc-
ument the title and all the clinical history, including
radiological findings, gross and microscopic descrip-
tions, etc. To get the expected output, we extracted
the top level MeSH diseases categories correspond-
ing to the diagnoses given on the titles of the “final
diagnosis” files (dx.html).
To select a proper ranking algorithm, we have
looked up the most suitable one through several
decades of literature about text classification and cat-
egory ranking. We have chosen the Sum of Weights
(SOW) approach (Ruiz-Rico et al., 2006), that is more
suitable than the rest for its simplicity, efficiency, ac-
curacy and incremental training capacity. Since med-
ical databases are frequently updated and they also
grow continuously, we have preferred using a fast and
unattended approach that lets us perform updates eas-
ily with no substantial performance degradation af-
ter incrementing the number of categories or training
samples. The restrictive complexity of other classi-
fiers such as SVM could derivate to an intractable
problem, as stated by (Ruch, 2005).
To evaluate how worth our suggestion is, we have
measured accuracy through three common ranking
performance measures (Ruiz-Rico et al., 2006): Pre-
cision at recall = 0 (P
r=0
), mean average precision
(AvgP) and Precision/Recall break even point (BEP).
Sometimes, only one diagnosis is valid for a partic-
ular patient. In these cases, P
r=0
let us quantify the
mistaken answers, since it indicates the proportion of
correct topics given at the top ranked position. To
know about the quality of the full ranking list, we use
the AvgP, since it goes down the arranged list averag-
ing precision until all possible answers are covered.
BEP is the value where precision equals recall, that
4
Data obtained on February 14th 2007
5
http://path.upmc.edu/cases
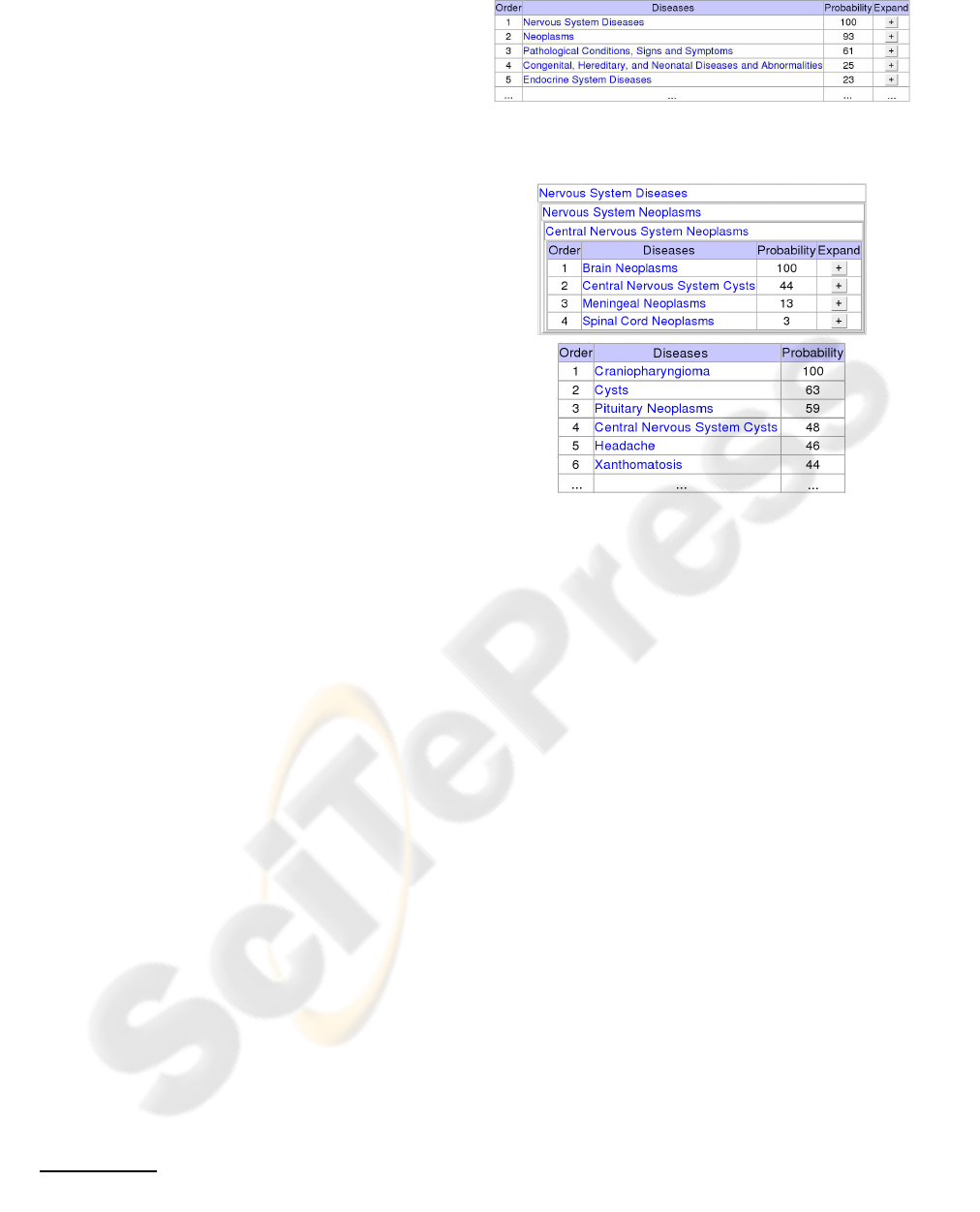
Figure 1: Example of the first level of a hierarchical diag-
nosis.
Figure 2: Output example after manual expansion of high
ranked topics (up) and by selecting the flat diagnosis mode
(down).
is, when we consider the maximum number of rele-
vant topics as a threshold. To follow the same proce-
dure as (Joachims, 1998), the performance evaluation
has been computed over the top diseases level.
2.1 Availability and Requirements
No special hardware nor software is necessary
to interact with the assistant. Just an Inter-
net connection and a standard browser are enough
to access on-line through the following site:
www.dlsi.ua.es/omda/index.php.
By using a web interface and by presenting re-
sults in text format, we allow users to access from
many types of portable devices (laptops, PDA’s, etc.).
Moreover, they will always have available the latest
version, with no need of installing specific applica-
tions nor software updates.
3 AN EXAMPLE
One of the 400 histories included in the test set looks
as follows:
Case 177 – Headaches, Lethargy and a Sel-
lar/Suprasellar Mass

A 16 year old female presented with two months
of progressively worsening headaches, lethargy and
visual disturbances. Her past medical history in-
cluded developmental delay, shunted hydrocephalus,
and tethered cord release ...
The final diagnosis expected for this clinical his-
tory is: “Rathke’s Cleft Cyst”, which is a synonym of
the preferred term “Central Nervous System Cysts”.
Translating this into one or several of the 23 top
MeSH diseases categories we are lead to the follow-
ing entries:
• Neoplasms
• Nervous System Diseases
• Congenital, Hereditary, and Neonatal Diseases
and Abnormalities.
In hierarchical mode, our approach provides auto-
matically a first categorization level with expanding
possibilities as shown in figure 1. We provide navi-
gation capabilities to allow the user to go down the
tree by selecting different branches, depending on the
given probabilities and his/her own criteria. More-
over, a flat diagnosis mode can be activated to directly
obtain a ranked list of all possible diseases, as shown
in figure 2.
After an individual evaluation of this case, we
have obtained the following values: P
r=0
= 1, AvgP =
0.92, and BEP = 0.67, since the right topics in figure
1 are given at positions 1, 2 and 4.
4 RESULTS
Last row in table 1 shows the performance measures
calculated for each medical history and its diagnosis,
averaged afterwards across all the 400 decisions. P
r=0
indicates that we get 69% of the histories correctly di-
agnosed with the top ranked MeSH entry. AvgP value
means that the rest of the list also contains quite valid
topics, since it reaches a value of 73%.
First row in table 1 provides a comparison be-
tween SVM (Joachims, 1998) and sum of weights
(Ruiz-Rico et al., 2006) algorithms using the well
known OHSUMED evaluation benchmark. Even us-
ing a training and test set containing different doc-
ument types, BEP indicates that the performance is
not far away from that achieved in text classification
tasks, meaning that category ranking can also be ef-
fectively applied to our scenario.
Table 1: Averaged performance for both text categorization
and diagnosis.
Corpus Algor. P
r=0
AvgP BEP
OHSUMED SVM - - 0.66
SOW - - 0.71
Case reports and
patient histories SOW 0.69 0.73 0.62
5 CONCLUSIONS
We believe that category ranking algorithms may pro-
vide a useful tool to help in medical diagnoses from
clinical histories. Although the output of the catego-
rization process should not be directly taken to diag-
nose a disease without a previous review, the accu-
racy achieved could be good enough to assist human
experts. Moreover, our implementation demonstrates
that both training and classification processes are very
fast, leading to an accessible and easy upgradable sys-
tem.
REFERENCES
Ibushi, K., Collier, N., and Tsujii, J. (1999). Classification
of medline abstracts. Genome Informatics, volume 10,
pages 290–291.
Joachims, T. (1998). Text categorization with support vec-
tor machines: learning with many relevant features. In
Proceedings of ECML-98, 10th European Conference
on Machine Learning, pages 137–142.
Ruch, P. (2005). Automatic assignment of biomedical cat-
egories: toward a generic approach. Bioinformatics,
volume 22 no. 6 2006, pages 658–664.
Ruiz-Rico, F., Vicedo, J. L., and Rubio-S´anchez, M.-C.
(2006). Newpar: an automatic feature selection and
weighting schema for category ranking. In Proceed-
ings of DocEng-06, 6th ACM symposium on Docu-
ment engineering, pages 128–137.
